In 10 years we can hope that local communities will start to welcome their own back as local medical specialists, writes Peter Hughes …
THE main objectives of the Regional Medical Specialists Association are to provide a forum for non-metropolitan specialists to discuss ways to improve conditions and equipment available, to encourage the highest standard of medical practice in regional areas and to assist in recruiting specialists to regional areas.
The first meeting of the RMSA was held in Canberra in May 2018, with attendees from Queensland, NSW, Canberra, Victoria and Tasmania. The second conference was held in Toowoomba, Queensland, in May 2019, and was very well attended. No conference was held in 2020 because of the COVID-19 restrictions, the 2021 conference in Orange, NSW and the 2022 conference in Wagga Wagga, NSW. The 2023 conference is planned for Port Macquarie, NSW and the 2024 conference for Mackay, Queensland.
About 28% of Australians live outside major Metropolitan centres1, yet the proportions of doctors living and working outside metropolitan areas is much less. This disproportion becomes stark when considering specialists.
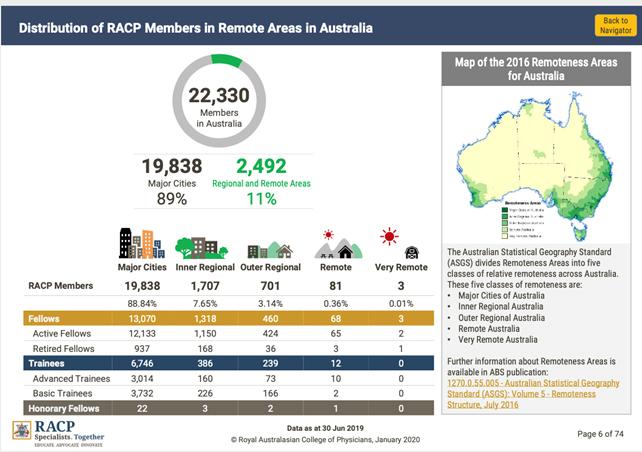
The above diagram from the Royal Australasian College of Physicians (RACP) shows that the maldistribution of practising physicians is mirrored by a maldistribution of trainees.
This pattern of maldistribution probably occurs in all of the surgical disciplines and psychiatry, although paediatrics has many vibrant regional training programs.
We specialists who live and work in regional Australia find it hard to understand how our metropolitan colleagues can’t see the advantages that we enjoy. We are part of a real community which is grateful for our presence and welcomes us into its embrace. Very little of our time is spent travelling, so we go straight from work to leisure with very little time wasted on the road. The majority of our regional hospitals have a supportive culture among colleagues. Continuing professional development is easy to maintain through in-house journal clubs, grand rounds and other clinical meetings. Life is good, real estate inexpensive and fresh food plentiful.
GPs provide most medical services to non-metropolitan patients. However regional centres in Australia must maintain general hospitals, staffed around the clock by specialists in various disciplines. The smaller hospitals rely on general physicians, general surgeons, general paediatricians and obstetricians/gynaecologists. Medium-sized to large regional hospitals can also support orthopaedics, oncology services, renal dialysis and mental health facilities.
But how to sustain such services when the vast majority of Australian medical graduates choose to live and work in the metropolitan areas? There is a limited future for specialty services without a continuous flush of trainees to refresh the workforce. Clearly this is not happening.
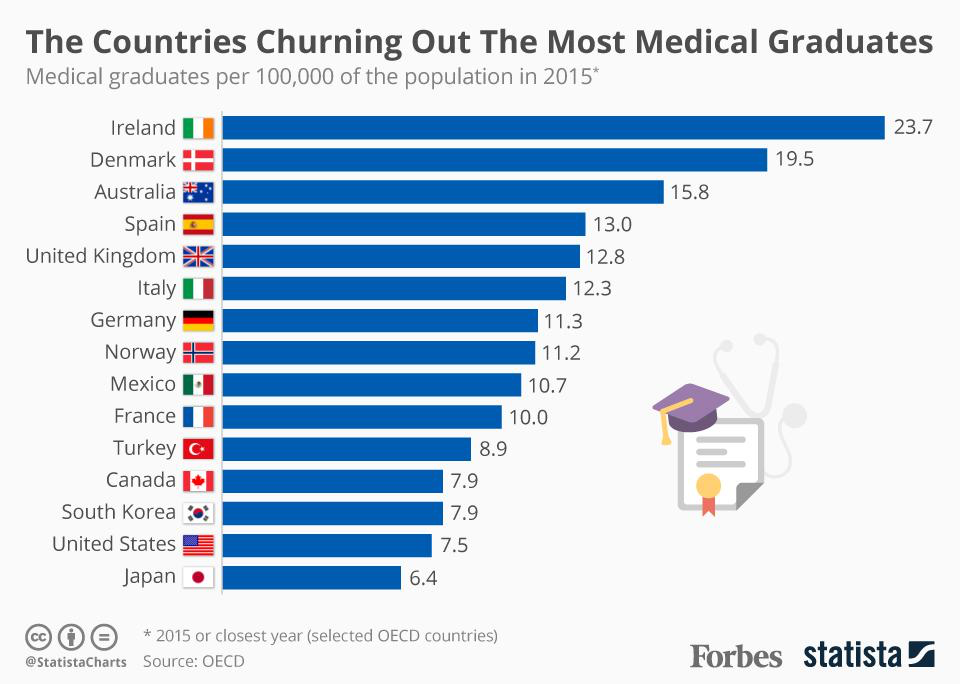
Our universities produce more medical graduates than almost any other OECD nation, yet our rural health services remain dependent upon international medical graduates (recruited from nations that can ill-afford to lose them) and the transient locum workforce.
The solution to this challenge must surely be to grow our own specialists in the regions. Sounds easy doesn’t it? It certainly is the aim of the Commonwealth’s Rural Health Multidisciplinary Training Program, and more recently the Integrated Rural Training Pipeline for Medicine (IRTP).
The IRTP was established by the Commonwealth in its 2015-16 Mid-Year Economic and Fiscal Outlook Statement. It is made up of three elements:
- The Regional Training Hubs, which are there to support and coordinate training of specialists in regional areas. Supervision and assessment of trainees remains the province of the Learned Colleges who are usually employed by the public hospital system;
- The rural junior doctor training innovation fund, which provides Commonwealth funding to support terms in rural general practice for interns and resident doctors; and
- Extra places quarantined in the Specialist Training Program (STP) for trainees spending at least two-thirds of their training time in non-metropolitan locations.
These interventions are backed by high-quality qualitative research here in Australia and overseas2. People born in rural areas are more likely to return to practice in a rural area3. Medical students who spend a year or more in a rural clinical school are more likely to return to practice in rural areas4. So also for graduates who complete their internship or at least a year of their post-graduate training in non-metropolitan centres.
It’s cheap and easy to blame the Learned Colleges for the lack of trainees in regional areas. The frequent, rather clichéd explanation offered is that the city professors want to keep the best and brightest on a short leash. The reality is in fact far more complex.
By the time a medical graduate is ready to enter specialist training he or she has spent at least 10 years in a metropolitan university or teaching hospital, in the majority of cases. Even those who were born in rural areas are conditioned to plan a future in the city. If they have met and married a city person, the partner is far less inclined to take the adventure to go rural than the other way around.
Accreditation of specialist training positions in rural and regional areas is difficult. In anaesthetics for instance, a particular case mix of surgical operations is needed for the anaesthetist to have all the skills quite rightly required by the college. In many medium to large regional areas, this full case mix is available, but only some of them in the public hospital system. Private hospitals and privately practising specialists have difficulty allocating time for teaching and supervision, and this time is not usually remunerated at all.
The specialist training program (STP) was originally designed to provide Commonwealth funding for specialist training in non-traditional metropolitan public hospital settings. Although rural settings are a good example of the above, metropolitan private hospitals, pathology laboratories and radiology practices were in a much better position to snap up these STP grants than rural hospitals.
The quarantined rural-based STP grants may help this, despite the constant case-mix challenge. Most of the Colleges are well aware of the inequity of health care that specialist maldistribution causes. They are genuinely trying to increase regional-based training, but the unpredictable case mix as well as the financial fragility of regional hospitals works against their best efforts.
The establishment of rurally-based “end-to-end” medical schools and the Integrated Rural Training Pipeline for Medicine together provide the best opportunity to make progress.
This package was proven successful in the Northern Ontario School of Medicine in the last decade. Local high school students, including indigenous students not able to leave their own country, can now aspire to a career in medicine, courtesy of a local entry-level medical school. Graduates can buy their first home during their rural hospital internship.
The regional training hubs will help provide innovative solutions to accreditation of more specialist Training posts. In 10 years we can hope that local communities will start to welcome their own back as local medical specialists.
“But the bush hath moods and changes,
as the seasons rise and fall,
And the men who know the bush-land
– they are loyal through it all.”
The Bulletin 23 July 1892. In Defence of the Bush
_______________
2Kondalsamy-Chennakesavan S, Eley DS, Ranmuthugal G, et al. Determinants of rural practice: positive interaction between rural background and rural undergraduate training. Med J Aust 2015; 202: 41-45.
3GT Somers, R Strasser, B Jolly What does it take? The influence of rural upbringing and sense of rural background on medical students’ intention to work in a rural environment Rural and Remote Health 7: 706. (Online), 2007 Available from: http://www.rrh.org.au
4Denese Playford Hanh Ngo Surabhi Gupta, Ian B Puddey Opting for rural practice: the influence of medical student origin, intention and immersion experience. Med J Aust 2017 207 (4) pp154-8..