The Regional Medical Specialists Association (RMSA) has issued a call for urgent action on
Medical Specialist services in Regional Australia.
This requires action by Commonwealth, specialist training institutions, State and Local
Government:
The Commonwealth needs to streamline its processes for allowing Internationally-Qualified Health
Practitioners (IQHPs) to gain entry into and registration in Australia;
Commonwealth and States must ensure that areas of medical workforce shortages are identified
as and when they occur;
Training institutions and rural communities must ensure that training and working as a medical
specialist in Regional Australia is seen to be attractive and rewarding.
Background
The RMSA was created in response to the chronic imbalance of medical specialist workforce between metropolitan cities and regional centres. This imbalance is worsening, not improving.
The Commonwealth’s responsibilities
An independent review of health practitioner regulatory settings was undertaken by Robyn Kruk AO. This report, endorsed by National Cabinet in December 2023, concludes that,
“…removing unnecessary regulatory barriers faced by IQHPs will improve care for Australians”.
The RMSA does not believe that international medical graduates are a permanent solution. However, urgent action is needed now to prevent any further degradation of rural health services.
Responsibilities of Specialist Colleges
The Medical Board of Australia, in response to the Kruk report, has consulted the Specialist Colleges to identify which overseas qualifications are suitable for ‘fast-tracking’ of applications by IQHPs. Good-faith responses are needed, and quickly. If the Specialist Colleges do not give guidance in this process it will happen without them.
In addition, the training colleges should set hard targets for the numbers of trainees working in rural areas. Medical specialist training should involve at least a year at a rural/regional location – ideally a third of the trainee’s time; proportionate to the population distribution.
States’ responsibilities
At the state level, more needs to be done to boost the financial viability and management expertise in rural hospitals. Public-private partnerships should be used more than they currently are to support specialist services in rural Australia. The Commonwealth and the States should ensure that methods for identifying medical workforce shortages are accurate and timely.
Local community responses
At the local community level, more effort is needed to make Regional and Rural centres more
attractive to newly-arrived medical trainees and specialists. This happens in some rural areas, but is not widespread.
Financial implications
The RMSA is not calling for financial incentives for individual doctors: this has been tried and failed. Rather, we call for better supports for trainees and specialists moving from metropolitan areas to regional centres. The cost of this support should be seen as investments in rural communities, for the benefit of all Australians.
Source material
Health inequity
Medical workforce imbalance creates dramatic health inequities between rural Australians and their city counterparts. Rates of cancer (see: Australian Cancer Council’s Australian Cancer Atlas) and heart disease (see: Heart Foundation’s interactive Heart Maps) rise the further a person lives away from a capital city: diagnosis is later and treatment less successful. Life expectancy falls with distance from Metropolitan centres, as shown by the Australian Institute of Health and Welfare.
This chart, from the Commonwealth’s Medical Workforce Data Sets, shows the dramatic reduction in medical specialists from Inner Metropolitan areas (Modified Monash Model 1) through inner regional areas (MM2) and beyond. This is not the distribution of the Australian population:
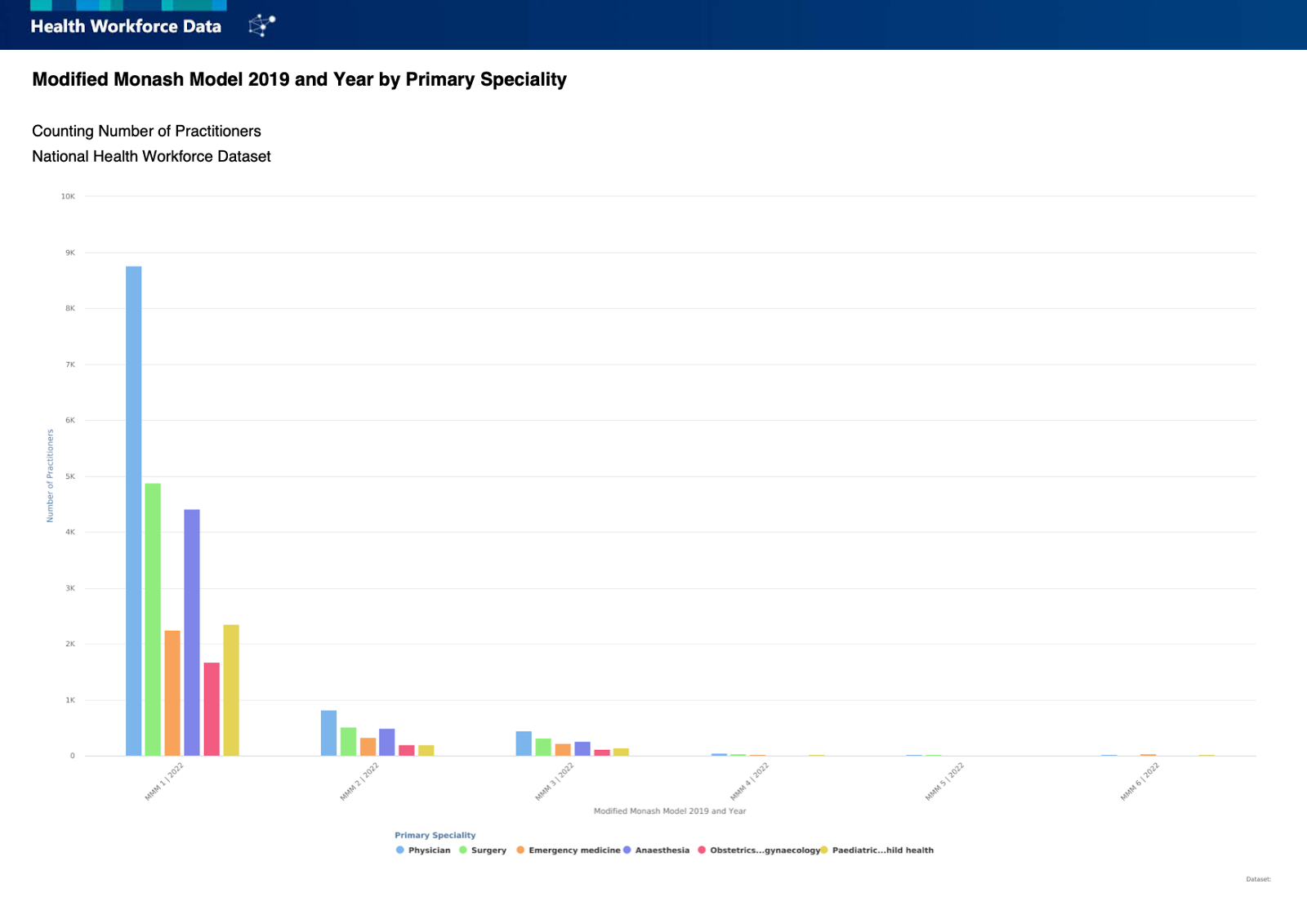
Despite the fact that over 30% of Australians live outside of Metropolitan areas, only 10% of
medical specialists live and work there. We cannot hope to improve the health outlook for rural
Australians unless this imbalance is fixed. People in rural Australia depend on local hospitals
staffed around the clock by specialist surgeons, physicians, obstetricians and paediatricians.
Urgent specialist medical workforce issues
In addition to chronic workforce shortages, several acute issues currently threaten services in regional centres. These centres are not recognised as districts of medical workforce shortage, as Medicare data are the main source of information used. Medicare data includes ‘outreach’, telehealth or temporary locum services in regional areas provided by specialists living in metropolitan areas. It does not accurately reflect the situation in regional communities.
Commonwealth initiatives on medical workforce
Commonwealth initiatives including the National Medical Workforce Strategy 2021-2031 and the
Rural Health Multidisciplinary Training Program aim to address these shortages. These will help in
the long-term, but not immediately. It takes at least 12 years to train a qualified medical specialist
from entry into Medical School.
A 2023 report by the Nous consultancy group demonstrated that government and NGO outlays on healthcare in the regions is $6.55 billion less per year than that in Metropolitan areas. This equates to a gap of $850 per person per year. This is despite the fact that regional Australia generates 80 percent of Australia’s export earnings – fisheries and forestry $76 billion and commodities $497 billion.